
Exophytic perianal nodule
With Anthony W. Linfante, MD, and Brent Kelly, MD
CASE HISTORY
A 52-year-old male Pacific Islander presented to the dermatology consult service with a 2-year history of a very slowly growing pigmented, exophytic perianal mass of about 2cm in diameter (Figure 1). The lesion was neither painful nor pruritic but did occasionally bleed. There was no history of prior significant trauma to the area. The patient denied a prior history of sexually transmitted diseases, including external genital warts. He had no prior personal history of cutaneous malignancy and was more or less immunocompetent.

The patient did have other health issues, including hyperlipidemia, hypertension, a past cerebrovascular accident, hepatitis C virus infection, hepatic cirrhosis, and a known patent foramen ovale. He was taking carvedilol 3.125mg twice daily and atorvastatin 10mg daily.
Over the course of his evaluation, diagnostic work-up was largely unremarkable except for expected laboratory abnormalities. Dermatoscopic examination revealed scattered foci of deep melanin-related hyperpigmentation, coarse arborizing blood vessels, and areas of fibrosis. As the differential diagnosis was broad, a tangential biopsy was performed, followed by a punch biopsy of the base of the lesion.
What do you think he has?
DISCUSSION
The differential diagnosis primarily included nodular melanoma, pigmented basal cell carcinoma (BCC), verruciform xanthoma, Buschke-Lowenstein tumor, external genital wart, condyloma lata, and chronic sinus tract. Skin biopsy revealed classic histology for pigmented BCC (Figure 2). The lesion was managed by wide local excision and primary closure.
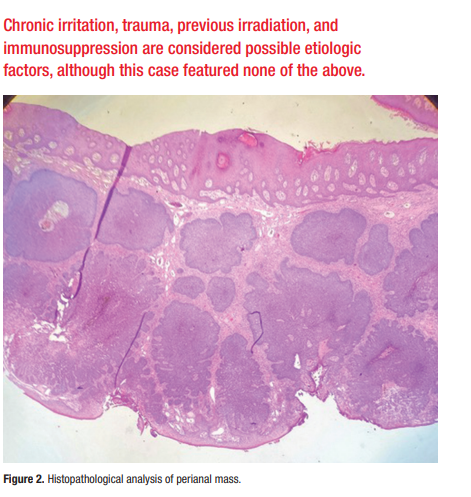
Perianal BCC is a rare tumor. Only about 0.08% of all BCC occur in this anatomic location. Conversely, only about 0.2% of all anorectal neoplasms are BCCs. The majority of such tumors occur in men of a mean age of 67. The clinico-histologic type is most often nodular, as in this case. Chronic irritation, trauma, previous irradiation, and immunosuppression are considered possible etiologic factors, although this case featured none of the above.
The National Comprehensive Cancer Network considers perianal BCC to be a “high risk” malignancy, and recommends removal via Mohs surgery. Nonetheless, smaller lesions (< 2cm) have also been successfully managed following wide local excision or radiotherapy.
This case was presented at the Texas Dermatological Society Spring Virtual Meeting, May 1, 2021.
Recommended reading: Aldana PC, et al. Perianal basal cell carcinoma successfully managed by excisional biopsy. Case Rep Dermatol Med. 2019 Jun 12; doi: 10.1155/2019/6268354.
